
ISOMETRIC LOAD PROGRESSION & TISSUE ADAPTATION RESEARCH
GRIPPŪL RESEARCH
WORKOUT LOAD AND FREQUENCY
Training at 70–80% of your measured MVC (maximum voluntary contraction) activates collagen synthesis and improves neuromuscular coordination for peak force expression. Studies confirm increased tendon stiffness and torque transfer in this range (link here). Avoid compensatory strategies like thumb wrapping when half-crimping—this recruits synergists and masks actual finger flexor output. Stay submaximal (never 100% MVC). Limit to 1–2 high-intensity sessions per week to allow tendon remodeling and prevent connective tissue breakdown. Every climber adapts differently based on limb length, tendon cross-sectional area, and sleep/nutrition. Some gain 2–5 lbs MVC/month, others 8–10 lbs. Respect your biology. Don’t chase numbers—prioritize rest, quality contraction, and progressive stimulus.
Training at 70–80% of your measured MVC (maximum voluntary contraction) activates collagen synthesis and improves neuromuscular coordination for peak force expression. Studies confirm increased tendon stiffness and torque transfer in this range (link here). Avoid compensatory strategies like thumb wrapping when half-crimping—this recruits synergists and masks actual finger flexor output. Stay submaximal (never 100% MVC). Limit to 1–2 high-intensity sessions per week to allow tendon remodeling and prevent connective tissue breakdown. Every climber adapts differently based on limb length, tendon cross-sectional area, and sleep/nutrition. Some gain 2–5 lbs MVC/month, others 8–10 lbs. Respect your biology. Don’t chase numbers—prioritize rest, quality contraction, and progressive stimulus.


Model/Athlete: Anika Westmark

REST BETWEEN REPS/SETS
Moderate & Easy
Reps rest: 1–2 seconds (neuromuscular potentiation focus)
Sets rest: 1–2 minutes (minimal phosphocreatine recovery)
For Intense
Reps rest: 5–10 seconds (ATP-PC recovery window)
Sets rest: 2–5 minutes (full phosphagen system reset)
PERIODIZATION
Adaptation depends on nervous system freshness and connective tissue remodeling. Use a 4-week progressive overload cycle to optimize collagen synthesis and force output. Week 1: 60% MVC, Week 2: 70%, Week 3: 80%, Week 4: deload back to 60%. After 4 weeks, retest MVC and recalculate intensities.
Moderate & Easy
Reps rest: 1–2 seconds (neuromuscular potentiation focus)
Sets rest: 1–2 minutes (minimal phosphocreatine recovery)
For Intense
Reps rest: 5–10 seconds (ATP-PC recovery window)
Sets rest: 2–5 minutes (full phosphagen system reset)
PERIODIZATION
Adaptation depends on nervous system freshness and connective tissue remodeling. Use a 4-week progressive overload cycle to optimize collagen synthesis and force output. Week 1: 60% MVC, Week 2: 70%, Week 3: 80%, Week 4: deload back to 60%. After 4 weeks, retest MVC and recalculate intensities.
CASE STUDY: Jonathan Xumo’s 3-Year Adaptation Trajectory
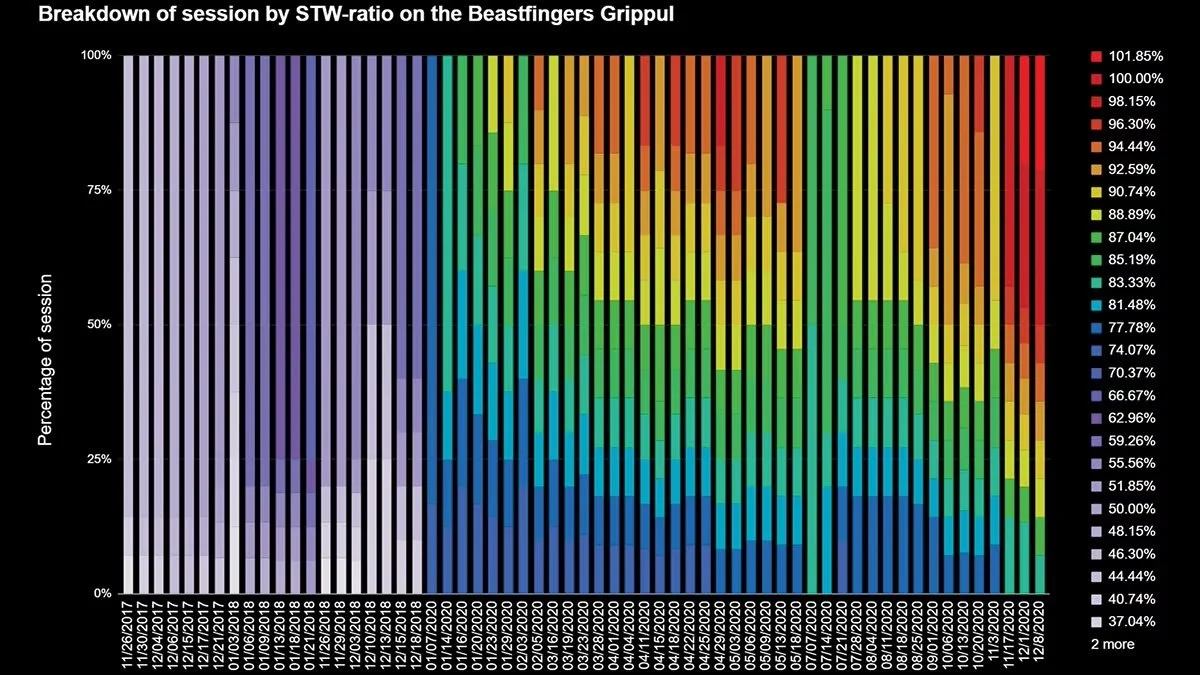
Athlete adaptation timelines are nonlinear and highly individualized. Jonathan Xumo initiated targeted strength training in November 2018 with a performance goal of outdoor V10. Despite 10+ years of climbing experience, his max outdoor boulder grade at that time was V7.
Beginning with a submaximal load protocol—training at ~50% bodyweight on a 20mm edge—he demonstrated consistent neuromuscular adaptation over time. By month 18, Xumo had progressed to producing 90% of his bodyweight on the same edge. Load progression was tightly controlled with autoregulated volume, yielding a net MVC gain rate of approximately 1.989 lb/month.
By the final quarter of his training arc, he demonstrated repeatable MVC values at 100% bodyweight on a 20mm edge—indicative of high tendon stiffness and efficient torque transfer. This phase coincided with a sharp increase in outdoor send grades, including The Occultist (V10, Connecticut) and two confirmed V9 ascents.
His current project is Krajo (V11, Gunks), where he’s executing full movement sequences and breaking the climb into two linked efforts—suggesting proximity to redpoint threshold. The data indicates that sustained high-intensity finger loading, when periodized and adjusted for RPE and recovery biomarkers, can lead to predictable tendon adaptation and strength translation into real-world climbing scenarios.
Athlete adaptation timelines are nonlinear and highly individualized. Jonathan Xumo initiated targeted strength training in November 2018 with a performance goal of outdoor V10. Despite 10+ years of climbing experience, his max outdoor boulder grade at that time was V7.
Beginning with a submaximal load protocol—training at ~50% bodyweight on a 20mm edge—he demonstrated consistent neuromuscular adaptation over time. By month 18, Xumo had progressed to producing 90% of his bodyweight on the same edge. Load progression was tightly controlled with autoregulated volume, yielding a net MVC gain rate of approximately 1.989 lb/month.
By the final quarter of his training arc, he demonstrated repeatable MVC values at 100% bodyweight on a 20mm edge—indicative of high tendon stiffness and efficient torque transfer. This phase coincided with a sharp increase in outdoor send grades, including The Occultist (V10, Connecticut) and two confirmed V9 ascents.
His current project is Krajo (V11, Gunks), where he’s executing full movement sequences and breaking the climb into two linked efforts—suggesting proximity to redpoint threshold. The data indicates that sustained high-intensity finger loading, when periodized and adjusted for RPE and recovery biomarkers, can lead to predictable tendon adaptation and strength translation into real-world climbing scenarios.
Strength Gains and the Menstrual Cycle
Training around the menstrual cycle helps the female athlete better understand fluctuations in her performance. My solution has been to provide varied stimulus to the fingers through all phases of the cycle, as well as use a campus board to stimulate adaptations on a skeletal level, further encouraging strength gains.
Most of your training gains will be during your follicular phase when progesterone is lowest. Week two into this phase, you’ll have a beneficial increase in testosterone and will feel your strongest—train hard! Testosterone helps accelerate collagen turnover and boost tendon strength.
When the luteal phase begins, force production will be lower, so focus more on recovery, stretching, nutrition, and endurance to help protect the tendons from injury.
Training around the menstrual cycle helps the female athlete better understand fluctuations in her performance. My solution has been to provide varied stimulus to the fingers through all phases of the cycle, as well as use a campus board to stimulate adaptations on a skeletal level, further encouraging strength gains.
Most of your training gains will be during your follicular phase when progesterone is lowest. Week two into this phase, you’ll have a beneficial increase in testosterone and will feel your strongest—train hard! Testosterone helps accelerate collagen turnover and boost tendon strength.
When the luteal phase begins, force production will be lower, so focus more on recovery, stretching, nutrition, and endurance to help protect the tendons from injury.
WARM-UP
Your warm-up should elevate tissue temperature, enhance tendon elasticity, and activate motor units without inducing fatigue. If you haven’t tested your MVC (Maximum Voluntary Contraction), you can estimate it based on your bodyweight and climbing grade using our calculator (here). Start with isometric hangs at ~50% of estimated MVC for 10s holds, 4 sets. Include general movement prep like push-ups or pull-ups (3 sets of 7) to prime large motor patterns. If climbing, low-grade bouldering or ARC-style traversing works as active warm-up.
Your warm-up should elevate tissue temperature, enhance tendon elasticity, and activate motor units without inducing fatigue. If you haven’t tested your MVC (Maximum Voluntary Contraction), you can estimate it based on your bodyweight and climbing grade using our calculator (here). Start with isometric hangs at ~50% of estimated MVC for 10s holds, 4 sets. Include general movement prep like push-ups or pull-ups (3 sets of 7) to prime large motor patterns. If climbing, low-grade bouldering or ARC-style traversing works as active warm-up.
Step 1: Find Your Max
Now we’ll find your starting point using the Rate of Perceived Effort (RPE) Scale, with 1-RPE being the easiest and 10-RPE being the hardest. First, warm up for 20 minutes with easy climbing at 3-RPE, and then take a 10- to 15-minute break. For the following tests, rest three to four minutes between sets; take as much rest as needed when attempting your 1RM.
Step 2: Calculate Your Training Weight
Your ideal training weight is 70 to 80 percent of your 1RM. For example, with a 1RM of 100 pounds on the 20 mm edge, your ideal range is 70–80 pounds.
Step 3: Workout Programming
Here’s a simple weekly model:
Now we’ll find your starting point using the Rate of Perceived Effort (RPE) Scale, with 1-RPE being the easiest and 10-RPE being the hardest. First, warm up for 20 minutes with easy climbing at 3-RPE, and then take a 10- to 15-minute break. For the following tests, rest three to four minutes between sets; take as much rest as needed when attempting your 1RM.
- 10 reps light weight (typically 40–60 lbs) at 2-RPE
- 9 reps moderate weight at 4-RPE
- 8 reps moderately heavy weight at 6-RPE
- 6 reps with a heavy weight at 7-RPE
- 2 reps with a heavier weight at 9-RPE
- 1 rep with an increased heavier weight at 10-RPE (assuming form is OK)
Step 2: Calculate Your Training Weight
Your ideal training weight is 70 to 80 percent of your 1RM. For example, with a 1RM of 100 pounds on the 20 mm edge, your ideal range is 70–80 pounds.
Step 3: Workout Programming
Here’s a simple weekly model:
- Intensity: 70 to 80 percent
- Workout: 3 sets of 7 lifts each
- Frequency: 2–3 days a week
- Re-test 1RM: Once a month or when recovered — gauge recovery via RPE. For example, if your workout weight was 70 lbs last week at 6-RPE, but is 55 lbs this week at 6-RPE, then dedicate more time to recovery.
Glossary
- 1RM (One-Rep Max): The maximum amount of force or weight a person can exert for a single repetition using proper technique.
- Absolute Strength: The peak force-generating capacity of the musculoskeletal system under maximal voluntary effort, regardless of time constraints.
- Collagen: The primary structural protein in connective tissues (e.g., tendons, ligaments), crucial for load transmission and tissue resilience under mechanical stress.
- DIP (Distal Interphalangeal Joint): The last joint of the finger, closest to the fingertip. Primary site of force application in isometric crimping. Often isolated in focused finger flexor training using tools like the Grippūl.
- PIP (Proximal Interphalangeal Joint): The middle finger joint. A key joint engaged in open hand and half-crimp positions. Excessive loading here without adaptation increases risk of pulley strain.
- MCP (Metacarpophalangeal Joint): The knuckle joint where the finger connects to the hand. Often stabilized during grip, but passive involvement can mask true finger flexor contribution.
- Mechanical Loading: The application of external force or strain to biological tissue, which may result in adaptive remodeling (e.g., increased tendon stiffness) or maladaptation (e.g., injury), depending on intensity, volume, and recovery.
- MVC (Maximum Voluntary Contraction): The greatest amount of force a muscle or group of muscles can voluntarily produce in a given movement. Used as the gold standard metric for finger strength testing.
- RFD (Rate of Force Development): The speed at which force can be produced. A key quality in dynamic or explosive climbing and campus board training.
- RPE (Rate of Perceived Exertion): A subjective metric for assessing training intensity, typically on a 1–10 scale, where 1 is minimal effort and 10 is maximum voluntary contraction or perceived failure.
- Tendon Force: The amount of force transmitted through a tendon during muscle contraction or external resistance, directly influencing tendon adaptation and strength output.
- Torque Transfer: The tendon's capacity to transmit rotational force from muscles to joints, enabling efficient lever-based movement across the skeletal system.

HEALTH DISCLAIMER
The material displayed on the Website is provided without any guarantees, conditions or warranties as to its accuracy. You should consult your physician or other health care professional before starting this or any other fitness program to determine if it is right for your needs. If you have any concerns or questions about your health, you should always consult with a physician or other health-care professional.



Featured








PACKAGE INCLUDES
Casted Aluminum Grippul (Textured).
20mm Black Quad Crimp (w/ 5/16” bolt)
FEATURES
Coated texture for better handling and friction.
Made of durable 6061 aluminum.
Compatible with standard climbing holds 3-5" wide.
Has 3 standard 3/8-16" threaded holes.
Load capacity tested ≈ Over 600 Lbs
Designed by Aman and Loophole Engineering.
InstructionsFinger CalculatorWorkouts
*Quad Crimp and bolt included. Tools Needed: 5/16” Hex wrench.